Lactate? Feeling the Burn.

In my recent article, “How Walking Can Save Your Life,” I give a short version of this article and practical tips for applying the knowledge.
The purpose of this article is to provide a more in-depth overview of the role of Lactate in the body, so that we can be intentional about training and exercise for everyone, from the metabolically disordered individual to the professional athlete. Many of the thoughts are derivations and compilations of key experts in this field. I think this is one of the most important (and most misunderstood) topics of the 21st Century. I will start with the sources:
Dr. Inigo San Millan (One of the Most Famous Students of Dr. George Brooks - Podcasts including both of them linked below)
Wait, what is Lactate? Dispelling Misconceptions about Lactate and Explaining the Lactate Shuttle
For most of my life, I was told lactate was toxic waste to my muscles and body, or “lactic acid” (colloquial term) was the thing that was making my calves tight during the school mile test. I remember vividly, crying because I didn’t reach the presidential standard in the mile test, and my coach telling me the “lactic acid” was the reason - while this wasn’t completely wrong, it wasn’t the full story.
Later in life as I got back into fitness, I discovered the real reason I couldn’t hold a high pace in the mile-test in school through the research by Iñigo San-Millán and his mentor, George Brooks, the lactate cycle, often referred to as the lactate shuttle, is a fundamental “bioenergetic” process in which lactate produced in one part of the body is transported to and consumed as a highly efficient fuel by another.
Lactate is primarily a vital cellular fuel. And the payoff is huge:
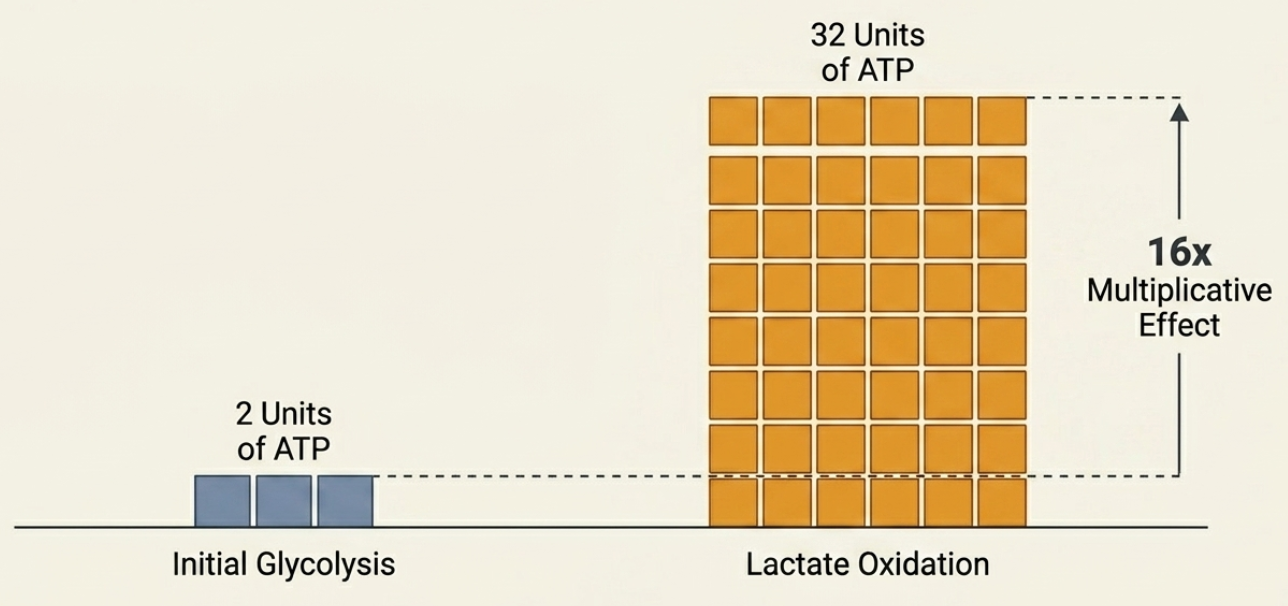
NotebookLM illustration of the energy result of the Lactate Shuttle
The cycle begins during glycolysis, the metabolic pathway cells use to break down glucose for rapid energy. As glucose is metabolized in the cell’s cytosol, it is converted into pyruvate.
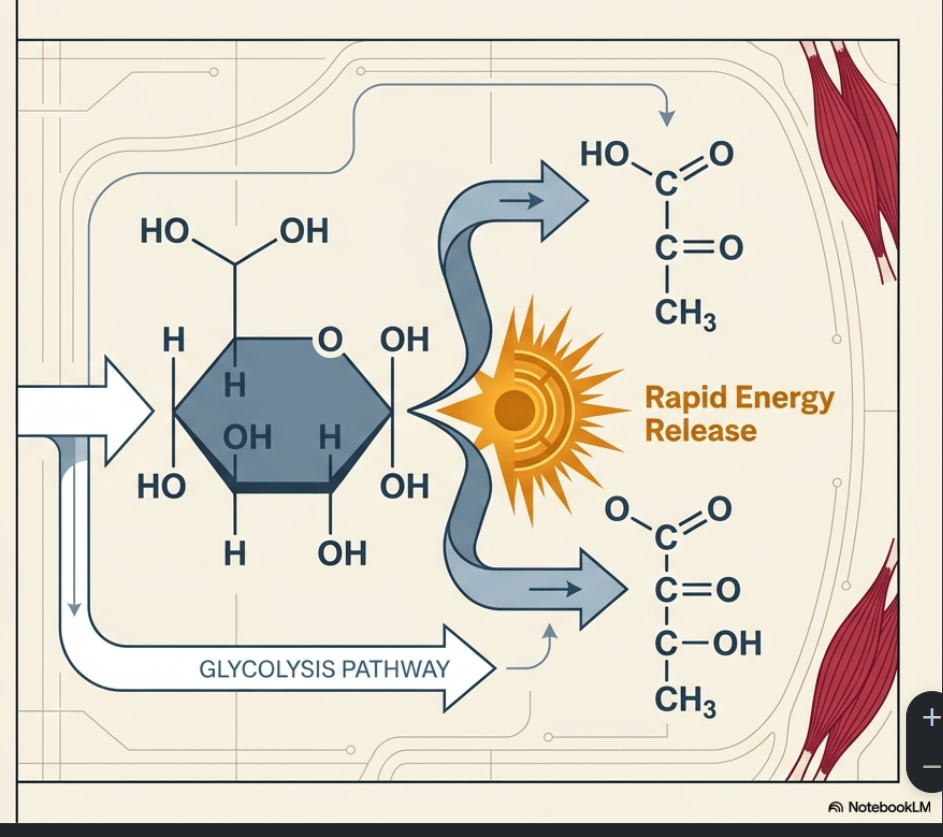
Using NotebookLM to illustrate (glucose on the left + pyruvate on the right side)
When cellular energy demand is high (such as during intense exercise), and there is a constant glycolytic flux, the cell consumes an essential coenzyme, NAD. For glycolysis to continue, the cell must constantly replenish its NAD supply, and it does so entirely by reducing pyruvate to lactate. Therefore, lactate is the mandatory and obligatory byproduct of glucose utilization.
Once produced, predominantly within highly glycolytic fast-twitch muscle fibers, lactate must go somewhere. If it cannot be used locally, it is actively exported out of the fast-twitch fibers via specific transporters called MCT4. From there, it either enters the systemic bloodstream or travels directly to adjacent, oxidatively capable slow-twitch muscle fibers.
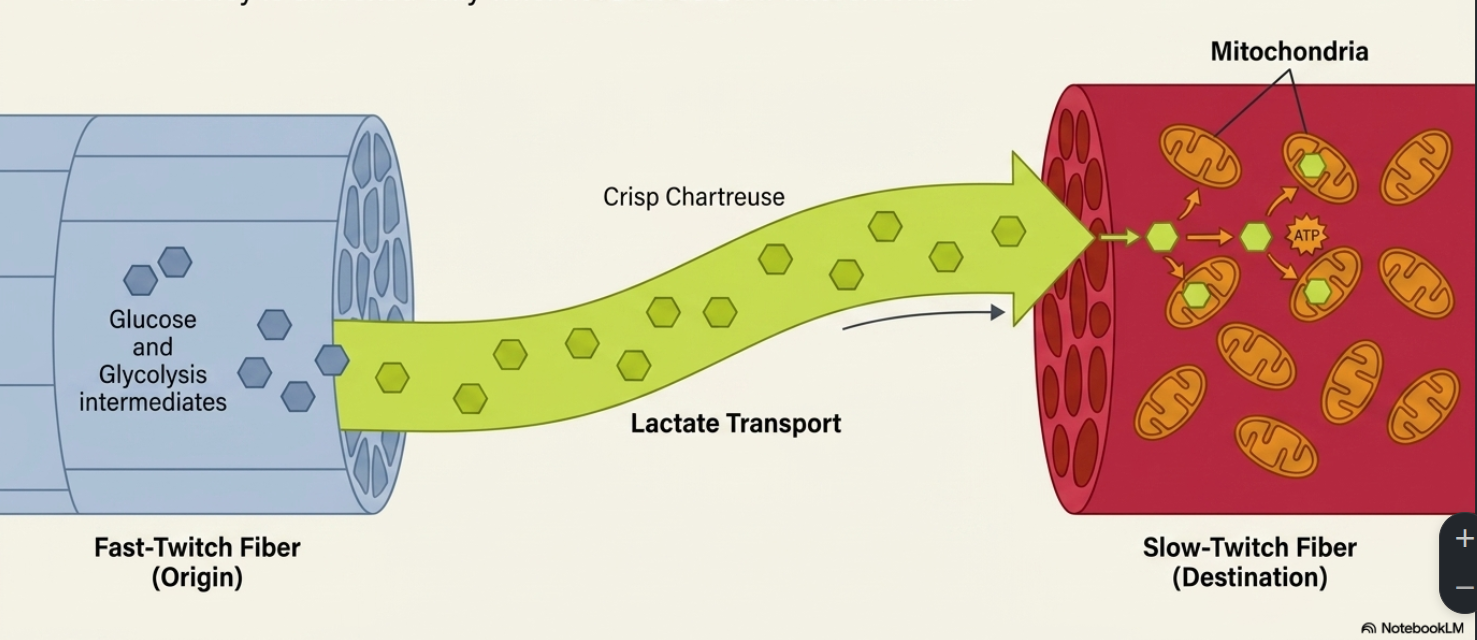
NotebookLM illustration of the Lactate Transport from Fast-Twitch Muscle Fibers to Slow-Twitch Muscle Fibers
The true efficiency of the lactate cycle is achieved when it reaches the slow-twitch muscle fibers and their mitochondria. Lactate enters the slow-twitch fibers and is transported into their mitochondria via the MCT1 transporter. Once inside the mitochondria, a specific enzyme called lactate dehydrogenase (LDH) oxidizes the lactate back into pyruvate. This pyruvate is then converted into Acetyl-CoA, which directly enters the Krebs cycle (oxidative phosphorylation) to produce massive amounts of energy. By recycling lactate through this cycle, the body generates highly efficient cellular energy, yielding 32 units of ATP instead of the mere two units generated during the initial breakdown of glucose.
Side Note on San-Millán’s Research: San-Millán’s work highlights that the capacity to efficiently shuttle and oxidize lactate is a profound marker of mitochondrial health and athletic performance. Elite athletes have trained their bodies to possess an extraordinary density of MCT1 transporters and highly functioning mitochondria.
Consequently, they can oxidize large amounts of lactate locally as fuel before it ever enters the bloodstream. This explains why an elite athlete’s blood lactate levels remain exceptionally low even at tremendous power outputs, whereas their actual local lactate production and clearance rates are incredibly high.
Conversely, individuals with metabolic syndrome, type 2 diabetes, or profound physical deconditioning suffer from severe mitochondrial dysfunction and lack the capacity to effectively run this cycle. When their poorly functioning bodies rely heavily on glucose and produce lactate, they lack sufficient MCT1 transporters or mitochondrial capacity to oxidize lactate. Because the lactate cannot be cleared locally, it mandatorily spills over into the bloodstream.
This lack of local clearance results in significantly elevated resting global blood lactate levels (sometimes between 1.5 and 3.0 millimoles) and rapid exhaustion during physical activity.
The accumulation of hydrogen ions associated with this uncleared lactate creates an acidic microenvironment that impairs muscle contractile force and velocity, thereby contributing significantly to rapid fatigue.
The Baseline of the Deconditioned Individual
Being metabolically deconditioned is specific. Specifically, we are referring to sedentary, overweight, and (possibly) diabetic individuals. Metabolic disorders can present themselves in a variety of ways, but the main takeaway is that there is metabolic dysfunction, specifically, there is mitochondrial dysfunction at the cellular level.
The first graph to understand is the one below, representing Blood-Lactate Levels:
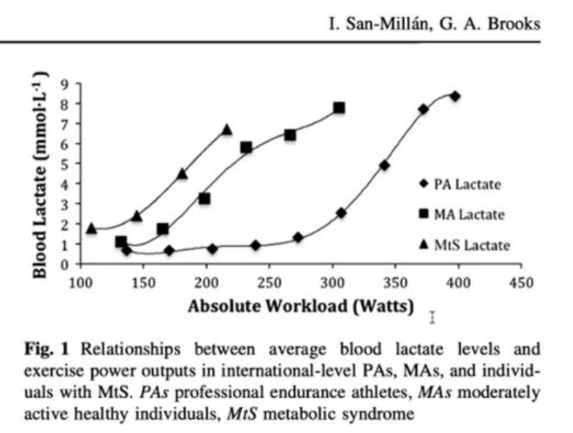
While this graph may look intimidating, let me draw your attention to the main points: 1) Let’s look at the triangles (representing MtS Lactate or Metabolic Syndrome population) at 100 Watts (or the equivalent of a brisk walk), there is more Lactate present in the blood than a Professional Athelete (PA represented by Diamonds) maintaining a 300 Watts workload (or the equivalent of a moderate to more intense steady-state exercise). 2) The most likely conclusion is that it is due to the Metabolic Syndrome individual's inability to utilize Lactate as fuel (or clear the lactate in the bloodstream due to this metabolic inefficiency & inflexibility).
Unconditioned individuals lack adequate mitochondrial capacity, meaning that lactate cannot be oxidized locally and is instead exported in large amounts into the bloodstream. Their bodies literally can not perform ideal energy processing.
Consequently, an unfit individual or someone with type 2 diabetes might exhibit resting blood lactate levels between 1.5 and 3.0 millimoles, which is significantly higher than the baseline of a fit individual, as seen above.
In my previous article, I talked about this lack of lactate clearance likely being the main reason extremely obese people (often 500+ pounds) report chronic global pain, the lactate itself is not the cause of the pain, but a cofounding sign of the likely true cause of the pain — hydrogen ions (a byproduct of the lactate shuttle that causes a lowering of pH first locally, then globally). When the body is unable to clear lactate, it is also unable to clear hydrogen, which accumulates and causes chronic global pain (at least that’s my hypothesis).
The graph below represents fat oxidation (FATox) across the same populations (or fat utilization as fuel for performance/work). This FATox graph is important to understand in relation to the Blood-Lactate (first graph) for many reasons: 1) It demonstrates that the Metabolic Syndrome Population is unable to utilize Fat as fuel in moderate intensity exercise. 2) It also demonstrates that the MtS population is unable to utilize Lactate or Fat as exercise intensity increases (leaving only Carbohydrates as a potential fuel source).
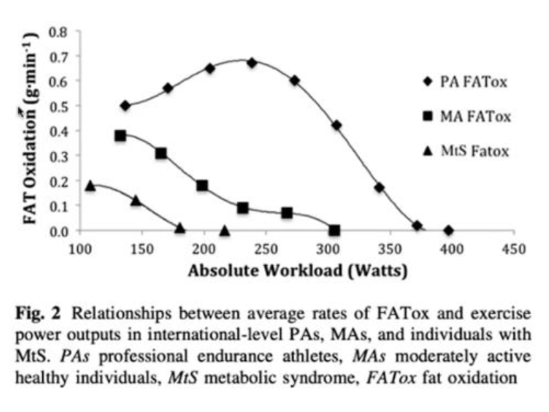
The conclusions to draw from these two graphs are the following: 1) The Metabolic Syndrome population can benefit immensely from low-impact steady-state exercise such as walking. And 2) as conditioning increases, so does metabolic flexibility, or as you get fitter, the better you are at utilizing Fat and Lactate as fuel in addition to carbohydrates.
Unfortunately, this means metabolic dysfunction is also characterized by the severe down-regulation of mitochondrial pyruvate carriers and fat transporters (CPT1 and CPT2).
This leads to an accumulation of stagnant intramuscular triglycerides that are high in ceramides, a known contributor to atherosclerosis and cardiometabolic disease. And increasing all-cause mortality dramatically.
The Role of Exercise as Cellular Medicine
Currently, there is no pharmaceutical pill that can directly increase mitochondrial function; exercise remains the only known “medication” to achieve this necessary adaptation.
Skeletal muscle is the primary battleground for metabolic health, as it oxidizes approximately 80% of the body’s carbohydrates. For individuals suffering from insulin resistance, the ability to translocate glucose transporters (GLUT4) to the cell surface to clear glucose from the blood is compromised.
Fortunately, muscle contraction provides a secondary, insulin-independent mechanism for glucose uptake. This means that physical activity can immediately begin pulling glucose from the bloodstream, making exercise, especially right after eating, a highly effective, non-pharmacological strategy for managing blood glucose levels.
Targeting Zone 2 to Rebuild the Metabolic Engine
To correct systemic metabolic issues, exercise must specifically target and stimulate the mitochondria without overwhelming the system. This is achieved through dedicated “Zone 2” training.
As we have covered previously, Zone 2 is defined as the exercise intensity at which you place the greatest stress on the mitochondria, primarily recruiting type 1 (slow-twitch) muscle fibers and mobilizing the highest amount of fat for energy. Training at this intensity stimulates the development of the cellular systems necessary for lactate clearance, including the proliferation of MCT1 transporters.
However, prescribing Zone 2 for an unconditioned person requires extreme care.
What could be an easy recovery pace for a professional athlete may be overwhelmingly stressful for someone with metabolic syndrome, pushing them out of fat-burning and into a purely glycolytic state almost instantly.
Therefore, a deconditioned individual may need to start at an exceptionally low power output, sometimes as low as 25-50 watts, to properly find their target fat-oxidation zone, in other words a very mild walk. As your conditioning improves, alongside your mitochondrial health, you will unlock higher levels to this “easy pace” for you.
Yours in Endurance,
MJ
Podcasts on the Topic:
Dr. George Brooks with Dr. Peter Attia